Osteogenesis imperfecta is a connective tissue disease characterized by extremely fragile bones due to an autosomal dominant genetic defect in type 1 collagen production. There are four main types of osteogenesis imperfecta: type I is the most common and the mildest form of the disorder, and is caused by an inadequate production of type 1 collagen. The remaining types are characterized by abnormal type 1 collagen formation. In addition to bone disorders, osteogenesis imperfecta is associated with blue sclera (Figure 1); lax ligaments; hearing impairments; facial abnormalities; short stature; scoliosis or kyphosis; and dental abnormalities.
Structure and Function
Osteogenesis imperfecta is a disease caused by a genetic mutation that causes abnormal type 1 collagen cross-linking. Patients either have insufficient production of type 1 collagen or they produce an abnormal version of type 1 collagen.
The lack of normal type 1 collagen leads to insufficient production of osteoid (the organic matrix of bone). The bones in osteogenesis imperfecta are brittle and fracture easily (hence the synonym “Brittle Bone Disease”). In some cases, the bones may be bowed or otherwise severely deformed.
Four main types of osteogenesis imperfecta have been identified. Osteogenesis imperfecta type I is the most common and mildest form; type II is the most severe. In most cases, osteogenesis imperfecta is inherited in an autosomal dominant pattern. Type III patients are most commonly seen in clinics because of their frequent fractures and need for surgery.
Although the name “osteogenesis imperfecta” implies imperfection (to say the least) in the bones, the disease can in fact affect all connective tissues in which type 1 collagen is found. Clinically, patients usually present with ligamentous laxity. Other clinical findings include basilar invagination of the skull (which may cause neurological symptoms), blue sclera, and abnormalities of the teeth (termed “dentinogenesis imperfecta”). Patients can also have structural abnormalities in and around the heart such as mitral valve prolapse and aortic dissection.
In the vast majority of cases, osteogenesis imperfecta results from a mutation in the COL1A1 or COL1A2 genes which encode proteins involved in the formation of type 1 collagen.
Mature collagen contains a large triple helix region in which two alpha1 chains (from the COL1A1 gene) and one alpha2 chain (from COL1A2) assemble together to form this triple helix. Normally, in the triple helix region of the chains, glycine occurs every third amino acid position in the chain in a glycine-X-Y pattern, where X and Y are frequently proline or hydroxyproline (Figure 2). This pattern allows the collagen fibrils to coil into the triple helix and helps define the unique biochemical properties of the protein.
Glycine is the simplest amino acid, with its side chain simply consisting of a hydrogen. With this simplicity, having glycine occur at every third spot in the amino acid chain allows the alpha chains to form a tight “twist.” This spatial arrangement wouldn’t otherwise be possible if an amino acid with a bulkier side chain were substituted for glycine.
In the most well-studied genetic abnormality in osteogenesis imperfecta, a point mutation in the COL1A1 and COL1A2 genes leads to the substitution of another amino acid in place of glycine. This impedes the correct association of alpha chains when forming the triple helix. This abnormal protein is then either hydrolyzed by the cell or simply fails to function properly.
Both autosomal dominant and autosomal recessive forms of the disease have been described.
Patient Presentation
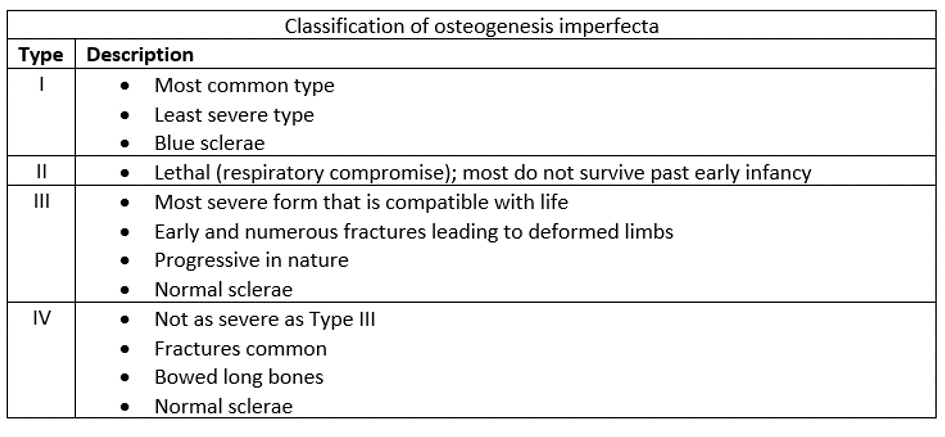
Any organ system in which type 1 collagen plays a structural role can be affected. The severity and phenotype vary widely depending on the type of osteogenesis imperfecta. While four types of osteogenesis imperfecta have been classically described (see Table 1), as many as 15 more have been added since.
Classically, patients with osteogenesis imperfecta have diminished growth. The face may have an atypical triangular shape, and the eyes may have blue sclera. The teeth are commonly affected, termed “dentinogenesis imperfecta,” due to abnormal dentin. This condition can lead to discolored, soft teeth with a predilection for dental caries. Hearing loss is commonly seen as well, which may be due to conduction abnormalities from the bones in the middle ear, sensorineural abnormalities from abnormalities of the inner ear organs, or a combination of the two.
The lungs and cardiovascular system may be affected. Patients with osteogenesis imperfecta can have abnormal valvular tissue leading to mitral valve prolapse or aortic regurgitation. The connective tissue of vessel walls is weakened which can lead to easy bruising.
Often musculoskeletal complaints will cause the patient to present to the orthopedist. Ligamentous laxity is characteristic, which leads to hypermobility of the joints. Basilar invagination, a condition in which the occipito-cervical junction gradually deforms and the edges of the foramen magnum fold inward, may be seen in some subtypes of osteogenesis imperfecta, leading to neurologic compromise. Scoliosis may be present to some degree, which may be quite severe in some subtypes.
Generalized bone brittleness and fragility are common. Recurrent fractures may lead one to suspect the diagnosis in otherwise mild forms of the disease. Olecranon apophyseal fractures are usually pathognomonic for osteogenesis imperfecta (Figure 3). Notably, the risk of fracture drops dramatically after puberty.
Severe bowing of the limbs is usually present in more severe forms (Figure 4A). The legs may exhibit the classic “saber shin” appearance due to anterior bowing of the tibiae (Figure 4B). The femora may be severely bowed. Compression fragility fractures of the spine lead to the classic “codfish vertebrae” appearance on lateral spine radio graphs (Figure 4C).
Objective Evidence
A diagnosis of osteogenesis imperfecta can usually be made based on family history and typical radiographic findings. Although DNA analysis may reveal mutations, especially in COL1A1 and COL1A2, due to the variety of mutations that lead to an osteogenesis imperfecta phenotype, there is no one simple lab test that can lead to diagnosis.
Radiographic analysis of patients with osteogenesis imperfecta will show osteopenia and thinned cortices. There may be radiographic evidence of multiple prior fractures – these may be pseudarthroses (a “false joint”) if the bones failed to heal.
Long bones are typically thin and have variable degrees of progressive bowing and general deformity. As mentioned above, the radiocapitellar joint may be dislocated, and ossification of the interosseous membrane can be seen. The pelvis may show coxa vara due to the stress seen at the proximal femur and an inability to remodel correctly in response to this stress.
In patients who have been treated with bisphosphonates, multiple radio-dense lines may be seen in long bones which correlate to growth arrest and subsequent recovery during treatment (Figure 5).
Multiple compression fractures in the spine may lead to a biconcave appearance of the vertebral bodies, the classic “codfish vertebrae” appearance, or even a complete flattening of the bone called platyspondyly (Figure 6) if the compression was more severe.
Basilar invagination can be evaluated with lateral cervical spine radiographs or sagittal views on CT scan or MRI. Basilar invagination is present when the dens protrudes superior to the McRae line, drawn from the caudal aspects of the basion and opisthion (Figure 7).
Epidemiology
Considering all subtypes, osteogenesis imperfecta occurs about once per 15,000–20,000 live births with no known variability across races and geographic regions. Type I osteogenesis imperfecta is the most common, found in one in 30,000 live births; osteogenesis imperfecta type II, the most severe form, is happily the rarest. Osteogenesis imperfecta affects males and females in equal numbers. In most cases, osteogenesis imperfecta is inherited in an autosomal dominant pattern. Osteogenesis imperfecta type II can occur as a spontaneous genetic mutation, which is then transmitted in an autosomal dominant pattern. Rare forms of osteogenesis imperfecta are inherited as autosomal recessive genetic traits.
Differential Diagnosis
Any disorder that presents with frequent or recurrent fractures may share some phenotypic characteristics with osteogenesis imperfecta. Importantly, if a child presents with multiple fractures, child abuse (non-accidental trauma) must be investigated and ruled out. Indeed, the possibility of child abuse must not be ignored merely because a diagnosis of osteogenesis imperfecta is present!
Other conditions which may have a musculoskeletal presentation similar to osteogenesis imperfecta include vitamin-D homeostasis deficiencies and hypophosphatasia, celiac disease, some forms of Ehlers-Danlos syndrome, Menkes disease, and I-cell disease.
Red Flags
- Any child presenting with skin lesions and/or fractures otherwise unexplained must be worked up for non-accidental trauma. As mentioned above, just because a diagnosis of osteogenesis imperfecta is made does not mean child abuse is not present
- Myelopathy or other motor/sensory changes, ataxia, decreased mental status, or apnea suggest possible basilar invagination.
- Easy fatigability, shortness of breath and murmurs must prompt an evaluation for mitral valve prolapse, aortic regurgitation, aortic dissection.
- The risk of malignant hyperthermia is increased in patients with osteogenesis imperfecta. Vigilance on the part of the anesthesia and surgical teams is required when patients are undergoing surgery.
Treatment Options and Outcomes
Treatment of the clinical effects of osteogenesis imperfecta is specific to each patient and subtype of disease. Many clinicians recommend early bracing to correct deformities and/or physical therapy in an effort to prevent fractures from occurring.
Bisphosphonates are also commonly used in patients with osteogenesis imperfecta, which have been shown to decrease the incidence of fractures as well as pain from impending fractures and brittle bones. Bisphosphonates work by inhibiting osteoclasts, which thereby effectively decreases bone resorption and leads to thicker cortical walls.
Certain fracture patterns treated non-operatively in children without osteogenesis imperfecta may also often be treated non-operatively in children with osteogenesis imperfecta. In an effort to prevent further fractures in this fragile population, the caveat with non-operative treatment is that light splints may be favored over rigid casts, and immobilization times generally are shortened.
Fractures of the femur and tibia may be treated with rods that span the entire bone to allow simultaneous support and continued growth. Load sharing devices that protect the whole bone should be used. Plates should be avoided due to the propensity for creating stress risers and increasing the risk of peri-implant fracture.
In the setting of bowed long-bones, single or multiple re-alignment osteotomies can be performed. These are secured with traditional (non-telescopic) rods (Rush) or telescopic rods (Fassier-Duval) which allow the rod to expand as the child continues to grow (Figure 8). A “bisphosphonate holiday” must be taken around the time leading up to long bone surgery and for some time thereafter, as bisphosphonates can impair the fracture and osteotomy healing process.
Basilar invagination, if severe, may be treated with surgical decompression and fusion from the occiput to either C2 or C3. This is done to prevent neurologic compromise. Scoliosis in children with osteogenesis imperfecta cannot be well controlled with bracing, as the bones are simply too fragile to allow that. Surgical fusion is sometimes performed when the curve progresses beyond 45 degrees, but may prove challenging due to the poor bone quality.
Life expectancy in osteogenesis imperfecta relates to the subtype of disease: Type II disease often results in perinatal death, whereas a normal lifespan can be expected in more mild Type I cases. Respiratory failure is the most common cause of death in patients with osteogenesis imperfecta.
Outcomes following fracture are poorer compared to the general population. The healing at the fracture site will not be as strong as fracture healing in an individual without osteogenesis imperfecta. This lack of strength is due to the defects in type I collagen and the important role that type I collagen plays in fracture remodeling.
Although patients with osteogenesis imperfecta experience a much higher fracture burden than the general population, most patients with the condition lead normal lives, work normal jobs, and have families. In general, patients with osteogenesis imperfecta should be counseled on optimizing bone health; this includes avoidance of smoking, excessive alcohol intake, appropriate calcium and vitamin D intake, and avoidance of high-risk activities that would put them an increased risk of skeletal trauma.
Risk Factors and Prevention
As osteogenesis imperfecta is a disease due to a genetic mutation, children of parents with known osteogenesis imperfecta are at higher risk of having the disease.
Respiratory failure (due to scoliosis, narrowed thorax, and basilar invagination) is the most common cause of death in patients with osteogenesis imperfecta.
Key Terms
osteogenesis imperfecta, COL1A1, COL1A2, blue sclera